About
The URBI study is designed to improve the way we screen for colon cancer in patients with ulcerative colitis and Crohn’s disease. Patients with these diseases are more likely to develop colon cancer than the general population. To lower this risk, doctors use colonoscopies to find and remove high-risk growths (also called polyps) before they turn into cancer. However, there is debate about how best to find and remove these precancerous growths in patients with ulcerative colitis and Crohn’s disease.
There is uncertainty about the practice of taking biopsies of areas that appear unlikely to have any precancerous changes (referred to as random biopsies). Some practice guidelines recommend taking lots of these biopsies during a colonoscopy. Other guidelines recommend against taking lots of random biopsies. This study aims to find out if taking these biopsies is helpful or harmful. Even expert doctors don’t know for sure if they are necessary.
The results of this study could change how colonoscopies are done and help create clear guidelines for the future. No matter what is found, we anticipate that this research will settle the debate and shape medical practice for patients with ulcerative colitis and Crohn’s disease.
Learn more about the URBI study by going to clinicaltrials.gov.
During a colonoscopy, your doctor may take a biopsy (sample) of the lining of the colon. The material collected is then prepared on a glass slide so that a pathologist can view the tissue under a microscope. Sometimes the biopsy is intended to remove an entire lesion from the colon. Other times the biopsy just takes a small sample of the area.
When doing a colonoscopy for patients with ulcerative colitis or Crohn’s disease, there are two main categories of biopsies that are collected:
Targeted biopsies are performed when the doctor identifies a suspicious appearing area. Depending on the size of the area and level of concern, the doctor will either obtain a small sample or remove the lesion completely.
Random biopsies are performed in areas where the doctor does not see any suspicious appearing changes. These biopsies are looking for microscopic changes that cannot be detected with colonoscopy alone.
Changes in Colonoscopy Technology and the History of Random Biopsies
The first modern colonoscopy was performed in 1969. In the 1980s and 1990s video colonoscopy was developed, allowing the doctor to view the colon on a large screen. Since that time, there have been many additional advances in colonoscopy technology and techniques. One of the most important advances was the introduction of high-definition imaging, similar to the advances in television images from the 1990s to today. This change made it easier to visualize small and subtle lesions that were often missed with earlier versions of colonoscopy.
The practice of taking multiple random biopsies throughout the colon as part of screening colonoscopy for patients with ulcerative colitis and Crohn’s disease dates back to the era before the availability of high-definition colonoscopy. Because the precancerous lesions were often difficult to see before the introduction of high-definition colonoscopy, the idea was that if the doctor obtained enough random biopsies, you might find the precancerous lesions by chance. When “invisible” precancerous lesions were found with random biopsies, patients were often recommended to have their colon removed.
Many gastroenterologists believe that lesions which were once considered “invisible” are now able to be seen with high-definition colonoscopy. This has drawn into question whether the practice of obtaining random biopsies is still helpful. One small research study from Japan suggested that the practice of obtaining many random biopsies may even reduce the ability to find the visible lesions but this question has not been definitively answered.
The URBI study will provide a more definitive answer to this question and will impact how colonoscopy is performed for patients with Crohn’s disease and ulcerative colitis.
Gangwani MK, Aziz A, Dahiya DS, Nawras M, Aziz M, Inamdar S. History of colonoscopy and technological advances: a narrative review. Transl Gastroenterol Hepatol. 2023 Apr 20;8:18. doi: 10.21037/tgh-23-4. PMID: 37197258; PMCID: PMC10184027.
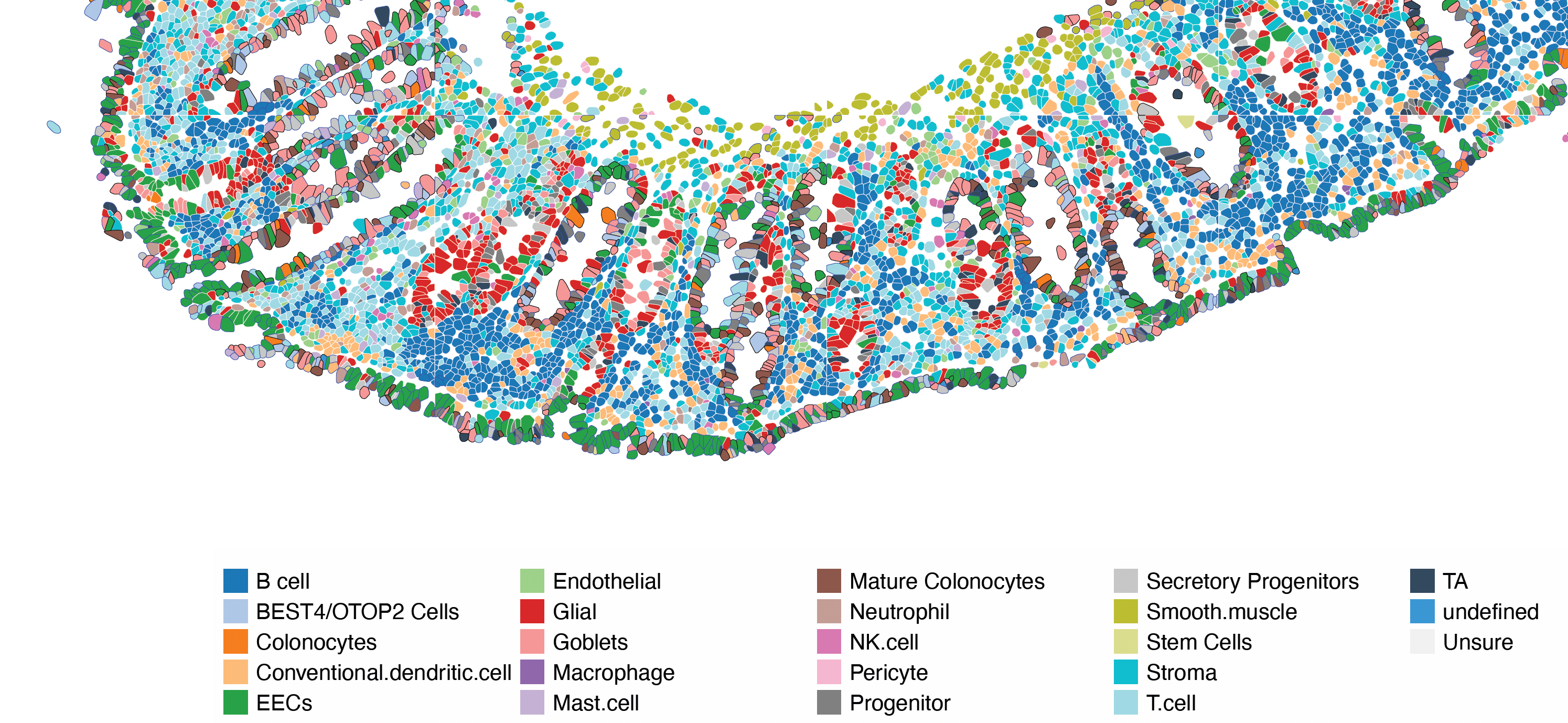
The intestine is made up of many different types of cells, each playing a crucial role. Some help with digestion and the absorption of food, while others protect us from infections. Immune cells, in particular, are very important in conditions like inflammatory bowel disease.
We are using a cutting-edge technology called spatial transcriptomics to examine all the cells in the colon lining. This technique allows us to see which genes are active in each cell, helping us identify the diverse types of cells that make up the human colon. The image shows some of these cell types discovered through our advanced methods. This innovative approach helps us create better diagnostic tools to assess inflammation levels, monitor how well treatments are working, and evaluate the risk of complications, especially colon cancer.